Pyloric stenosis
Granskad av Dr Toni Hazell, MRCGPSenast uppdaterad av Dr Philippa Vincent, MRCGPLast updated 18 Nov 2024
Uppfyller patientens redaktionella riktlinjer
- Ladda nerLadda ner
- Dela
- Language
- Diskussion
- Ljudversion
- Add to preferred sources on Google
Pyloric stenosis affects between 2 and 5 out of 1,000 newborn babies. It causes a blockage of food at the stomach outlet (pylorus). The main symptom is projectile vomiting after every meal causing weight loss and dehydration. A small operation is needed, which cures the problem.
At a glance
Pyloric stenosis is a condition where the outlet of a baby's stomach is narrowed.
It typically affects babies between 2 and 6 weeks old.
The main symptom is forceful, projectile vomiting after feeds.
Affected babies may not gain weight and can become dehydrated.
A small operation can usually cure the problem.
Seek medical advice if your baby has persistent forceful vomiting.
I den här artikeln:
Video picks for Baby och småbarn
Fortsätt läsa nedan
What is pyloric stenosis?
pyloric stenosis
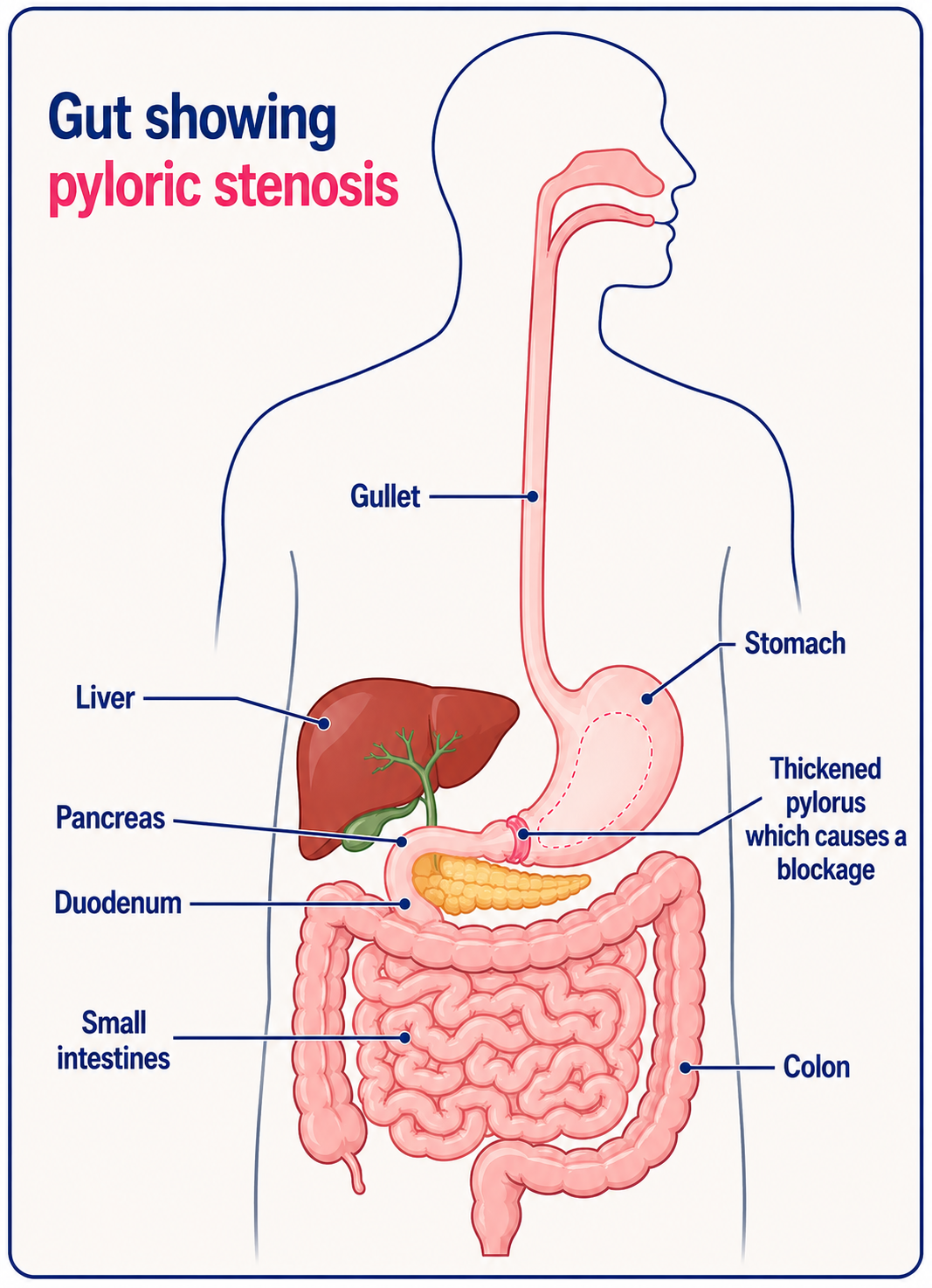
The outlet of the stomach into the small intestine is called the pylorus. Stenosis means a narrowing. Pyloric stenosis means a narrowed outlet of the stomach.
Food and drink pass down the gullet (oesophagus) into the stomach. Here the food and drink mixes with acid and are partially digested. The stomach then normally passes the food and drink into the small intestine to be fully digested and absorbed into the body.
When the outlet from the stomach into the small intestine is narrowed this causes a serious illness unless it is treated.
What are the symptoms of pyloric stenosis?
Tillbaka till innehållSymptoms typically begin in a baby aged between 2 and 6 weeks who is otherwise healthy.
Vomiting after a feed is the main symptom. The vomiting may start like a 'normal' vomit but often the vomiting is forceful and milk may be vomited quite a distance like a fountain. This is called projectile vomiting.
The baby remains alert and hungry, and will usually feed well - only to vomit the milk back soon after feeding. The vomiting tends to become worse and worse over several days.
Little food or drink passes through the narrowed pylorus which becomes narrower over time. This means that little or no food reaches the bowels, so babies often pass very little faeces (poo). Affected babies do not gain weight, and are in danger of quickly becoming dehydrated and seriously ill if the condition is not treated.
Notera: it is very common for newborn babies to vomit. The vast majority of babies who vomit do inte have pyloric stenosis.
Fortsätt läsa nedan
What causes pyloric stenosis?
Tillbaka till innehållThe muscle in the wall of the outlet of the stomach into the small intestine (pylorus) is abnormally thick. This causes the outlet from the stomach to become narrowed (stenosed). It is not known why this occurs though some risk factors have been identified. Use of a particular type of antibiotic shortly after birth has been shown to be a risk factor for developing pyloric stenosis.
Pyloric stenosis affects between 2 and 5 out of 1,000 babies. Boys are affected more commonly than girls. It can sometimes run in families. It is more common in babies who are bottle fed, who were born by caesarean section or who were born prematurely. It is more common in first-born babies. It is also more common in babies born to women who smoked during pregnancy.
It is seen most commonly in white babies and less frequently in Black or Asian babies.
Are any tests needed for pyloric stenosis?
Tillbaka till innehållOften the story is enough to make a doctor suspect the diagnosis of pyloric stenosis. A doctor may examine the baby's abdomen whilst they are feeding. A typical bulge next to the stomach can sometimes be felt as the muscles in the stomach and stomach outlet (pylorus) contract.
An ultrasound scan may be done if there is doubt about the diagnosis. This painless test is very reliable at detecting the thickened pylorus. Possibly because ultrasound is being used more frequently, pyloric stenosis is being diagnosed earlier and fewer babies are becoming very unwell before being diagnosed.
Fortsätt läsa nedan
What is the treatment for pyloric stenosis?
Tillbaka till innehållA small operation, done under a general anaesthetic, normally cures the problem. A small cut is made in the skin over the stomach outlet (pylorus) and the pylorus itself is then cut to create a channel for food to pass through. This operation is called a pyloromyotomy.
Food and milk can then pass easily out of the stomach into the bowel.
A pyloromyotomy is now usually done by keyhole surgery. This uses only a tiny cut to the skin to allow fine instruments into the abdomen to cut the pylorus muscle.
The operation is usually totally successful. Normal feeds are started again shortly after the operation. Most babies recover quickly and have no further problems.
Can pyloric stenosis be prevented?
Tillbaka till innehållPyloric stenosis cannot be prevented. Although there are certain risk factors which might make it more likely, there is always a combination of factors causing pyloric stenosis so it cannot be prevented.
Patient picks for Baby och småbarn

Barnhälsa
Undescended testicles
An undescended testicle (testis) is more common in boys who are born prematurely. Although in the majority of cases the testicle descends by the age of 6 months, some boys will need an operation. This is called an orchidopexy. This operation brings the testicle down from the tummy (abdomen) into the testicular sac (scrotum). There is an increased risk of infertility and also cancer if the testicle remains in the abdomen.
av Dr Laurence Knott

Barnhälsa
Erythema toxicum neonatorum
Erythema toxicum neonatorum (ETN) is a common skin rash affecting healthy newborn babies. It is not serious, does not cause the baby any harm and clears up without any treatment. It is sometimes known as erythema toxicum, baby acne or toxic erythema of the newborn.
by Dr Hayley Willacy, FRCGP
Vanliga frågor
My baby vomits after feeding; how can I tell if it's normal or if it could be pyloric stenosis?
Many newborns vomit, and it's usually normal. However, if your baby's vomiting becomes increasingly forceful, like 'projectile vomiting' where milk is vomited a significant distance, and they remain hungry but don't gain weight, this can be a sign of pyloric stenosis. If you are concerned, it's best to seek medical advice.
Could my baby be diagnosed with pyloric stenosis if they are older than 6 weeks?
Symptoms of pyloric stenosis typically begin in babies aged between 2 and 6 weeks. While the article notes this is the typical age range, it doesn't exclude the possibility of diagnosis outside this window, but it is less common.
My baby is bottle-fed. Does this increase their risk of pyloric stenosis?
Yes, pyloric stenosis is more common in babies who are bottle-fed. Other risk factors include being a first-born baby, being born by caesarean section or prematurely, having a mother who smoked during pregnancy, and a family history of the condition. Boys are also affected more often than girls.
How quickly can my baby recover after the surgery for pyloric stenosis?
Most babies recover quickly after the pyloromyotomy operation. Normal feeds can usually be started again shortly after the procedure, and most babies have no further problems.
What happens if pyloric stenosis is not treated?
If pyloric stenosis is not treated, it can lead to a serious illness. The baby will not gain weight and is at risk of quickly becoming dehydrated, as little food or drink can pass through the narrowed stomach outlet to be absorbed by the body.
Will my baby need a large cut for the operation?
A pyloromyotomy, the operation to correct pyloric stenosis, is now usually performed by keyhole surgery. This method involves only a tiny cut to the skin to allow fine instruments to be used, rather than a large incision.
How reliable is an ultrasound scan for diagnosing pyloric stenosis?
An ultrasound scan is a very reliable and painless test for detecting the thickened pylorus muscle, which is characteristic of pyloric stenosis. Its increased use has led to earlier diagnoses.
Vidare läsning och referenser
- Galea R, Said E; Infantile Hypertrophic Pyloric Stenosis: An Epidemiological Review. Neonatal Netw. 2018 Jul;37(4):197-204. doi: 10.1891/0730-0832.37.4.197. Epub 2018 Jul 1.
- Garfield K, Sergent SR; Pyloric Stenosis.
Fortsätt läsa nedan
About the authorView full bio

Dr Philippa Vincent, MRCGP
General Practitioner, Medical Author
MB BS, Bsc, MRCGP (2000), DCH, DFSRH, DRCOG
Dr Philippa Vincent is an NHS GP working in North London.
About the reviewerView full bio

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell qualified from St. Mary’s Hospital Medical School and did her VTS at Northwick Park Hospital.
Artikelhistorik
Informationen på denna sida är skriven och granskad av kvalificerade kliniker.
Next review due: 17 Nov 2027
18 Nov 2024 | Senaste versionen

Fråga, dela, anslut.
Bläddra i diskussioner, ställ frågor och dela erfarenheter inom hundratals hälsorelaterade ämnen.

Känner du dig sjuk?
Bedöm dina symtom online gratis
Anmäl dig till Patientens nyhetsbrev
Din veckovisa dos av tydliga, pålitliga hälsoråd - skrivna för att hjälpa dig känna dig informerad, självsäker och i kontroll.
By subscribing you accept our Sekretesspolicy. Du kan avsluta prenumerationen när som helst. Vi säljer aldrig dina uppgifter.