Tarm polyper
Colonic polyps
Granskad av Dr Colin Tidy, MRCGPSenast uppdaterad av Dr Toni Hazell, MRCGPSenast uppdaterad 15 Sept 2023
Uppfyller patientens redaktionella riktlinjer
- Ladda nerLadda ner
- Dela
- Language
- Diskussion
- Ljudversion
- Lägg till i föredragna källor på Google
I denna serie:TjocktarmscancerTjocktarmscancerscreeningFekalt immunokemiskt testSigmoidoskopiKolonoskopiCT-kolonografi
Bowel polyps (colonic polyps) are small non-cancerous (benign) growths on the inside lining of the bowel (colon and rectum).
Överblick
En tarmpolyp är en liten, godartad tillväxt inuti tarmen.
De flesta tarmpolyper orsakar inga symtom.
Vissa adenompolyper har en liten risk att bli cancerösa över flera år.
De flesta tarmpolyper kan tas bort under en koloskopi.
En hälsosam livsstil kan hjälpa till att minska risken för att utveckla polyper.
What are bowel polyps?
A bowel polyp is a small non-cancerous growth. There are many types of polyps, such as those that occur in the nose - this leaflet is about polyps that occur in the bowel.
Types of bowel polyps
Large bowel - polyp
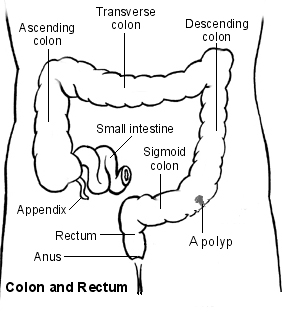
Most bowel polyps develop in the part of the colon called the descending colon, which leads down to the rectum. However, they can occur anywhere in the colon or rectum. Bowel polyps can be divided into three types: hyperplastic polyps, adenomas and polyposis syndromes.
Hyperplastic bowel polyps
These are a common type of bowel polyps. They are small - usually less than half a centimetre in diameter. They are generally regarded as harmless and only very rarely turn into cancer.
Adenomas
These too are a common type of bowel polyp. Most are small (usually less than a centimetre in diameter) but they can be bigger. There is a small risk that an adenoma may, in time, become cancerous. If one does turn cancerous, the change usually takes place after a number of years.
The relationship between polyps and cancer is that most bowel cancers (colorectal cancers) develop from a polyp that has been present for 5-15 years. In other words, although most adenomas do not become cancerous, the vast majority of cancers in the bowel initially develop from an adenoma that has been present for a number of years.
It is difficult to be certain of the exact risk of developing cancer from an adenoma. One study suggested that for a single 1 cm adenoma, the risk of it turning cancerous was about 1 in 12 after 10 years, and about a 1 in 4 after 20 years. However, the risk seems to vary depending on factors such as the size of the adenoma and the exact type of adenoma.
There are different types of adenoma and some types are more likely than others to develop into bowel cancer. See also the separate leaflet on Tjocktarmscancerscreening.
Polyposis syndromes
Polyposis syndromes are a group of inherited conditions. They include:
Familial adenomatous polyposis (FAP).
Hereditary nonpolyposis colorectal cancer (HNPCC)/Lynch's syndrome.
Gardner's syndrome.
Turcot's syndrome.
Peutz-Jeghers syndrome.
Cowden's disease.
Familial juvenile polyposis.
Hyperplastic polyposis.
These are rare syndromes. They cause polyps in young people and often cause multiple bowel polyps that have a high chance of developing into bowel cancer.
Bowel polyp symptoms
Most people with one or more bowel polyps do not have any symptoms. Most people who have a bowel polyp will never know they have one.
However, some people with bowel polyps will get symptoms. Polyps do not usually cause abdominal pain or a change in bowel habits. Symptoms include:
Blood in the stools (faeces). There may also be mucus in the stools.
Diarré eller constipation, but this is much less likely than blood in the stools. Diarrhoea or constipation is much more likely to have a cause other than a bowel polyp.
Causes of bowel polyps
The lining of the bowel constantly renews itself throughout our lives. New cells are made in the lining of the bowel and these cells eventually die to be replaced by more new cells. Each of these cells contains genes which control how the cell works.
Family history may play a role, because if the gene doesn't work properly then some cells may grow more quickly. This may eventually cause a polyp to develop. Some faulty genes cause a tendency for the lining of the bowel to develop polyps or bowel cancer, which may be inherited from our parents.
How common are bowel polyps?
Bowel polyps are really common in older people. About 1 in 4 people over the age of 50 years develop at least one colonic polyp. Bowel polyps are much less common in younger people.
Some people develop just one bowel polyp. It is not uncommon to have two or more. However, having more than five polyps is unusual.
Riskfaktorer
Risk factors include increasing age, being overweight and smoking. If you have a family history of a bowel polyp or cancer, or have had either of these yourself in the past, you are also at higher risk. Another risk factor is having inflammatory bowel disease (ulcerative colitis or Crohn's disease).
Diagnosing bowel polyps
Most bowel (colonic) polyps do not cause symptoms. So, most people with bowel polyps will not be diagnosed. Screening tests may be done if you have symptoms that indicate a bowel problem, or for various other reasons. For example, if you have seen blood in your stools (faeces) or if you are found to have blood in your stools following a routine screening test which is now offered to older people.
See the separate leaflet called Faecal Occult Blood Test for more details.
Vad är en koloskopi?
Most bowel polyps are diagnosed by this procedure. Colonoscopy is a test where an operator - a doctor or a nurse - looks into your colon. A colonoscope is a thin, flexible telescope. It is about as thick as a little finger. It is passed through the anus and into the colon. It can be pushed all the way around the colon as far as the caecum (where the small and large intestine meet). The colonoscope contains fibre-optic channels which allow light to shine down so the operator can see inside your colon.
See the separate leaflet called Colonoscopy for more details.
A sample (biopsy) will be taken at the time of the colonoscopy. This is very important so that it can be checked whether the polyp is cancerous (malignant).
What about other tests?
Sometimes a bowel polyp is diagnosed by other tests:
A special X-ray test of the bowel - this procedure is called a barium enema.
A CT colonogram - air and a contrast dye are pumped into the bowel to make the anatomy clearer to see and you are then examined by a CT scanner.
A test procedure called sigmoidoscopy - this enables a doctor or nurse to use an instrument called a sigmoidoscope to look into the rectum and sigmoid colon. The procedure is similar to a colonoscopy but it uses a shorter telescope.
If a bowel polyp is seen on a barium enema or CT colonogram you will still need a colonoscopy to remove the polyp and to take a sample (biopsy) of it for further investigation. The advantage of a colonoscopy as the first test is that the biopsy can be taken and/or the polyp removed all at the same time.
You will also need a colonoscopy if a polyp is found when you have a sigmoidoscopy. This is to make sure there are no more polyps beyond the reach of sigmoidoscopy.
Treatments for bowel polyps
If you are diagnosed with a bowel polyp, you will usually be advised to have it removed, even if it is not causing any symptoms. This is because there is a small risk of the polyp developing into a cancerous (malignant) growth at some time in the future.
Kolonoskopi
Most bowel polyps can be removed during a colonoscopy. The colonoscope has a side channel down which a grabbing device can be passed. This device can be manipulated by the operator. The operator can therefore see and also remove a polyp during a colonoscopy. The removal of the polyp is usually painless. Once removed, the bowel/colon polyp is sent to the laboratory to be looked at under a microscope. This is done to check:
That it has been completely removed.
The type of polyp.
Whether it is non-cancerous (benign) or showing signs of cancerous (malignant) change.
Most removed polyps will show full removal and be totally benign.
Your consultant will advise on the need for follow-up. This may depend on factors such as the size of the bowel polyp, the exact type of polyp that has been removed, the laboratory report about the polyp, and your age. Once these factors are considered, some people are advised to have regular colonoscopies in the future to make sure no more bowel polyps develop. As with any test, the results should be given to you by the team who arranged the test. So if you are not sure about how to access the results, phone or email your consultant's secretary, not your GP.
Kirurgi
If you have many bowel polyps (especially if you have a polyposis syndrome) then you may need to have an operation to remove part of your bowel. This is because it isn't possible to completely remove all the bowel polyps by using colonoscopy.
Preventing bowel polyps
Polyps cannot be prevented, but a healthy lifestyle (not smoking and not being overweight) can help to reduce your risk.
Patientval för Bowel problems

Matsmältningshälsa
Gastrointestinal malabsorption
Gastrointestinal malabsorption syndrome means a failure to fully absorb digested foods from the gut (bowel) into your body. There are many different causes. Prolonged intestinal malabsorption may cause problems because of a lack of carbohydrates, proteins, fats, minerals and vitamins that are essential to keep you healthy. The treatment will depend on the cause of malabsorption but will also include supplements and other ways to make up for the reduced amount of carbohydrate, protein, fat, minerals and vitamins getting into your gastrointestinal tract.
av Dr Hayley Willacy, FRCGP

Matsmältningshälsa
Inflammatorisk tarmsjukdom
Inflammatorisk tarmsjukdom (IBD) är en term som används för att beskriva personer som har någon av de två huvudtyperna av IBD (Crohns sjukdom och ulcerös kolit). Båda dessa tillstånd kan orsaka inflammation i tjocktarmen och ändtarmen (tjocktarmen eller grovtarmen) med liknande symtom, såsom blodig diarré, magont (buksmärta), viktminskning och dålig aptit.
av Dr Colin Tidy, MRCGP
Vanliga frågor
Var förekommer tarmpolyper vanligtvis?
Tarm polyper utvecklas oftast i den nedåtgående tjocktarmen, som leder till ändtarmen. De kan dock bildas var som helst i tjocktarmen eller ändtarmen.
Vad är den typiska storleken på hyperplastiska tarmpolyper och adenom?
Hyperplastiska polyper är vanligtvis små, vanligtvis mindre än en halv centimeter i diameter. Adenom är också ofta små, vanligtvis mindre än en centimeter, men de kan ibland bli större.
Vad är ett 'polyposis syndrom'?
Polyposis syndromer är en grupp ovanliga, ärftliga tillstånd som orsakar polyper att bildas, ofta hos unga människor, och involverar vanligtvis flera tarmpolyper med en hög risk att utvecklas till tarmcancer. Exempel inkluderar Familjär adenomatös polypos (FAP) och Lynchs syndrom.
Vad händer efter att en tarmpolyp har tagits bort under en koloskopi?
När en tarm polyp har tagits bort, skickas den till ett laboratorium för undersökning under mikroskop. Detta görs för att bekräfta att den har tagits bort helt, för att identifiera dess typ och för att kontrollera om den är godartad eller visar tecken på cancerförändring.
Behöver jag uppföljningsbesök efter att en tarmpolyp har tagits bort?
Din konsult kommer att ge råd om uppföljning behövs. Detta beror på faktorer som storleken och typen av den borttagna polypen, laboratorieanalysrapporten och din ålder. Vissa personer kan bli rekommenderade att genomgå regelbundna koloskopier i framtiden för att övervaka nya polyper.
Vidare läsning och referenser
- Combined endoscopic and laparoscopic removal of colonic polyps; NICE Interventional procedures guidance, September 2014
- Colorectal cancer (management in people aged 18 and over); NICE Guidance (2020, last updated December 2021)
- Bowel screening; NICE CKS, May 2019 (UK access only)
- Bonnington SN, Rutter MD; Surveillance of colonic polyps: Are we getting it right? World J Gastroenterol. 2016 Feb 14;22(6):1925-34. doi: 10.3748/wjg.v22.i6.1925.
Om författarenVisa fullständig biografi

Dr Toni Hazell, MRCGP
MBBS, BSc, MRCGP, DFSRH, Dip GU med, DRCOG, DCH (London, UK, 2000)
Dr. Toni Hazell tog examen från St. Mary’s Hospital Medical School och genomförde sin VTS vid Northwick Park Hospital.
Om recensentenVisa fullständig biografi

Dr Colin Tidy, MRCGP
Allmänläkare, Medicinsk Författare
MBBS, MRCGP, MRCP (Paediatrics), DCH
Dr Colin Tidy är en NHS-läkare, baserad i Oxfordshire.
Artikelhistorik
Informationen på denna sida är skriven och granskad av kvalificerade kliniker.
Artikeln finns också på Engelska, Tyska, Spanska, Franska, Italienska, Portugisiska, Hindi, Hebreiska, Arabiska, och Svenska.
Next review due: 13 Sept 2028
15 Sept 2023 | Senaste versionen

Fråga, dela, anslut.
Bläddra i diskussioner, ställ frågor och dela erfarenheter inom hundratals hälsorelaterade ämnen.

Känner du dig sjuk?
Bedöm dina symtom online gratis
Anmäl dig till Patientens nyhetsbrev
Din veckovisa dos av tydliga, pålitliga hälsoråd - skrivna för att hjälpa dig känna dig informerad, självsäker och i kontroll.
Genom att prenumerera accepterar du våra Sekretesspolicy. Du kan avsluta prenumerationen när som helst. Vi säljer aldrig dina uppgifter.
Mer om matsmältningshälsa
- Acid reflux och esofagit
- Antispasmodika
- Bariumlavemang
- Tjocktarmscancerscreening
- Campylobacter
- Kronisk pankreatit
- Celiaki
- Crohns sjukdom
- Diarrémedicin
- Matförgiftning hos barn
- Gallstenar
- Gastrointestinal malabsorption
- H2-blockerare
- Helicobacter pylori
- Smärta i vänster nedre kvadrant
- Leversvikt
- Alkoholrelaterad fettlever
- Bukspottkörtelcancer
- Primär biliär kolangit
- Shigella